
What is corneal cross-linking?
Corneal cross linking, also known as corneal collagen cross linking, was first introduced in the late 1990s as a form of treatment to slow down or arrest the progression of keratoconus. Cross linking works by increasing the number of collagen bonds in corneal tissue, thereby strengthening the cornea and maintaining its structural integrity.
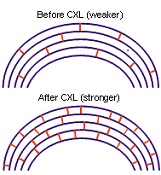
Corneal collagen fibers play an important in maintaining the shape and structure of the cornea. Collagen bonds interlink the collagen fibers with each other, thus holding the fibers together. Increasing the number of collagen bonds will benefit eyes where there are insufficient bonds to maintain the normal shape and structure of the cornea. This happens in corneal diseases such as keratoconus or as a complication after LASIK.
If performed early enough, corneal cross linking can strengthen the cornea enough to avoid further weakening and change in shape. This helps to preserve visual function, limit further visual deterioration, and postpone or even avoid more invasive surgery such as corneal transplant surgery.
Although widely performed throughout the world, including the United States, cross linking treatment has still not received approval from the Food and Drug Administration (FDA). Major clinical trials are currently being conducted in the US and Australia to provide evidence for the efficacy of this treatment.
What does corneal cross linking involve?
Corneal collagen cross linking is a straightforward and non-invasive day case procedure that takes around 60 to 90 minutes. It is done under topical anesthesia, i.e. you will only require anesthetic eye drops. You will not need any anesthetic injections or to undergo general anesthesia.
During the procedure, your corneal epithelium (the outermost layer of the cornea, or ‘skin’ of the cornea) is gently removed. Riboflavin 0.1% (vitamin B2) drops are are then applied at intervals of 1 to 5 minutes for up to 30 minutes. Enough riboflavin has been applied if it can been seen in the anterior chamber of the eye using the blue filter on slit lamp examination. The riboflavin acts as a photosensitizing agent.
Once the riboflavin has been adequately absorbed into the cornea, ultraviolet light A (typically in the 365 to 370 micrometer wavelength range) is applied 1 to 5 cm from the cornea for 30 minutes (see right). During UVA irradiation, the riboflavin solution will still be periodically applied onto the cornea.

At the end of the procedure, a bandage contact lens may be placed to improve comfort and to help the epithelium to grow back. This takes around 2 to 3 days. You will also be given antibiotic and anti-inflammatory eye drops to reduce the risk of infection and to settle the post-procedure inflammation.
You can also have cross linking performed without having your epithelium removed. In transepithelial corneal cross linking, the corneal epithelial surface is left intact. Because the epithelium acts as a natural barrier, a longer riboflavin loading time will be required compared to epithelium-off cross linking. In Europe, a special riboflavin formulation, Ricolin TE, has been developed to enhance transepithelial cross linking.
What to expect after corneal cross linking
For the first few days after cross linking, your eyes will feel uncomfortable and scratchy. This will ease as the corneal epithelium heals. Once the epithelium heals, your vision should return to what it was before the procedure, and the bandage contact lens can be removed. For the best results, make sure you instil the eye drops as instructed by your ophthalmologist.
Current research has shown that the corneal shape will remain stable or achieve improvement 99% of the time, up to a period of 1 year. In most cases, the keratoconus does not worsen and in some cases, the vision may improve. You may return to wearing contact lenses after one month. However, the contact lenses that you wear may need to be changed occasionally until the cornea fully stabilizes.
Corneal cross linking is a relatively safe procedure. The concentration of riboflavin and radiation dose of UVA used in cross linking are safe and do not cause damage to the cornea, lens or retina However, some complications have been reported following treatment, including:
– Corneal haze and edema
– Corneal scarring
– Infection
In terms of visual outcomes, both epithelium-off cross linking and transepithelial cross linking show similar results. However, transepithelial cross linking may have the added advantage of more rapid healing, faster visual recovery, less discomfort and reduced risk of infection and corneal haze.
Suitability for corneal cross linking
Not everyone with keratoconus or corneal ectasia from LASIK is suitable for corneal collagen cross linking treatment. Factors that need to be considered include the stage and severity of the disease as well as the rate of progression.
One of the most important considerations is the thickness of the cornea. Only corneas that have a thickness greater than 400 micrometers are suitable. If your cornea is less than 400 micrometers thick, there is a risk that the corneal endothelium (innermost lining of the cornea) can become damaged by the UV irradiation. Damage to the corneal endothelium may then lead to corneal edema, resulting in haziness of the cornea and reduced vision.


{kind=link}